Intro to Extended Streamline Tractography
Diffusion tensor imaging (DTI) has become a mainstay in today’s neuroimaging research toolbox. It is essential for in vivo study of white matter pathways in structural neuroimaging. It is however hampered by its inability to resolve crossing fibers within key brain regions. This limitation is due to the DTI gaussian diffusion model, where regions of low anisotropy and cross-fiber regions are indistinguishable due to their gaussian diffusion profile.
A number of approaches has appeared over the years to better image crossing regions. Most of these approaches are based on diffusion acquistions of more than 50 directions, and therefore belongs to the category of high angular resolution diffusion imaging (HARDI). Newer approaches tend to fall into model-free or model-based methods. Where model-free methods attempts to estimate a number of direction maximums directly from the diffusion signal, while model-based methods attempts to estimate a set number (generally less than 3) of fiber directions by simplifying the underlying diffusion assumptions. Due to the fact that these methods are all trying to estimate multiple fiber directions, sometimes they are called multi-tensor methods, although the term is not exacly correct, as a number of these methods do not estimate tensors at all.
Due to the higher complexity of model-free methods, they are sensitive to acquisition quality. Often times they rely on a different sampling scheme in q-space, such as cartesian grid sampling in diffusion spectral imaging (DSI), or more popularly radial sampling on single or multiple concentric spherical shells such as in Q-ball and Constrined Spherical Deconvolution (CSD).
XST
Extended Streamline Tractography (XST) is a 2-tensor tractography algorithm developed by Qazi et al. It is hidden away as part of the TEEM library, but it’s a very capable tractography algorithm.
We have experimented with a number of tractography methods, and have found ourselves always return to XST for most of our tractography applications. This is due to a number of reasons.
- Acquisition limitation, as it’s nearly impossible to convince the hospital accept research protocols such as multi-shell on a clinical scanner.
- Patients cannot tolerate the long scanning times, and we have to accomadate other clinical MR acqusitions in the same time block.
- Increased false positives from other methods that may be a result of the nature of the algrithm and compounded with our data acquisition limits.
XST is a more conservative method when comparing to CSD, as evident on the 2015 Tractogram results.
| Method | VB / 25 | IB / 2450 | VC (%) | VCWP (%) | IC (%) | NC (%) | Mean crossing angular error (degrees) |
|---|---|---|---|---|---|---|---|
| CSD step=0.1 | 23 | 259 | 64.70 | 0.67 | 20.61 | 14.02 | 23.35 |
| CSD step=0.5 | 23 | 251 | 69.92 | 0.56 | 19.79 | 9.73 | 23.67 |
| XST step=0.3 | 23 | 183 | 59.05 | 1.80 | 17.29 | 21.86 | 22.21 |
VB: Valid bundle; IB: Invalid bundle; VC: Valid connection; VCWP: Valid connections through a wrong path; IC: Invalid connection; NC: No connection
One thing to note is the larger percentage of NC for XST. Once we understand how XST works, the result is not suprising as we’ll see later.
Under the hood
XST makes the assumption that there are at most 2 crossing fibers directions per voxel. The second tensor direction is constrained to the plane defined by the first two diffusion eigen vectors $\hat{e}_1$,$\hat{e}_2$, and the second diffusion tensor perpendicular and parallel diffusions are identical to the first.
The Westin diffusion measures (Westin et al, 2002) are derived from diffusion eigen magnitudes, and include three measures:
The alternative formulation for these equations are:
Intuitively the westin anisotropy measures can be visualized thus as glyphs (Kindlemann, 2004):

The availability of the second tensor is then determined by the Westin planarity index $C_p$, as only sufficiently planar diffusion estimate can confidently estimate the second direction.
The diffusion profile in grey matter is highly isotropic, and therefore would result in high $C_s$, low $C_p$ and $C_l$. It’s therefore not suprising that XST will not extend as far into the cortical grey matter regions compare to CSD, and therefore has a higher NC score as mentioned earlier.
Example applications
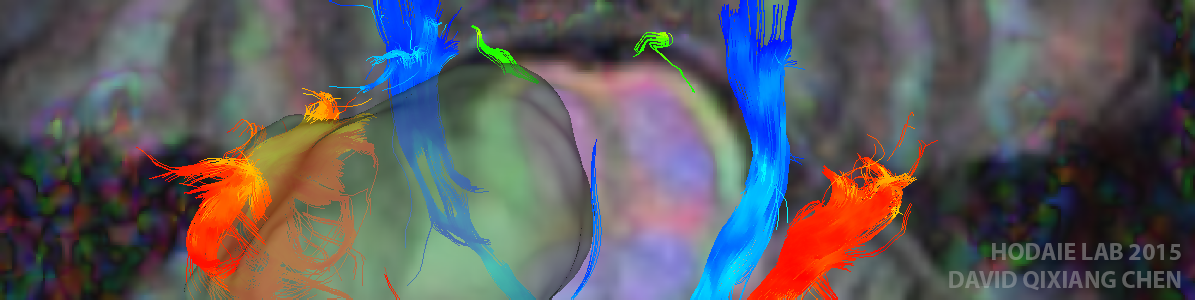
We have found that XST lends itself especially well to cranial nerve tractography (Chen et al, 2015). Its more conservative nature makes it easier to visualize nerves even in case of pathology.

Improvements
The TEEM XST implementation is single threaded, and therefore running time was very slow. Jasmine Quigley implemented parallelization of the tracking algorithm that greatly speed up the running time. We have published our parallelized XST on Github.
Before Parallelization:

After Parallelization:

Installation
In Ubuntu 12.04 and above, make sure that you have packages build-essentials, cmake, and cmake-curses-gui.
You can find our fork of TEEM on Github, or run:
git clone https://github.com/sinkpoint/hodaie-teem.git
Once cloned, run:
mkdir build
cd build
ccmake ..
Then follow instruction to configure and generate the makefile, then run:
make
sudo make install
To install the binaries
Usage
XST is part of the tend command. To use it, call
tend fiber -i dwi.nhdr -dwi -wspo -ns seeds.txt -o output.vtk -ap \
-t 2evec0 -stop aniso:cl2,0.2 frac:0.1 radius:0.8 minlen:10 -n rk4 \
-k cubic:0.0,0.5 \
-v 2 -step 0.3
The important parameters are:
-t 2evec0: Set the tractography algorithm to XST.-ns seeds.txt: Supply a list of N3 coordinates in world space as initial seeding points.-wspo: Output the tracts in world space.-stop aniso:? frac:? radius:? minlen:?: The XST parameters, aniso can be any one of the westin measures, and there are 2 versions of each.
Caveats
There a number of limits of the current implementation of XST that one needs to be aware of:
- Only one b=0 volume can be present in the input dwi file.
- Input NRRD file should be encoded in RAS coordinate frame.
References
-
Chen, D.Q., DeSouza, D.D., Hayes, D.J., Davis, K.D., O’Connor, P., Hodaie, M., 2015. Diffusivity signatures characterize trigeminal neuralgia associated with multiple sclerosis. Mult. Scler. J. 1–13. doi:10.1177/1352458515579440
-
Qazi, A.A., Radmanesh, A., O’Donnell, L., Kindlmann, G., Peled, S., Whalen, S., Westin, C.-F., Golby, A.J., 2009. Resolving crossings in the corticospinal tract by two-tensor streamline tractography: Method and clinical assessment using fMRI. Neuroimage 47 Suppl 2, T98–106. doi:10.1016/j.neuroimage.2008.06.034
-
Westin, C.-F., Maier, S.E., Mamata, H., Nabavi, a, Jolesz, F. a, Kikinis, R., 2002. Processing and visualization for diffusion tensor MRI. Med. Image Anal. 6, 93–108.